Throwback Thursday, March 18, 2021
In today’s edition of Throwback Thursday, I’m thrilled to include Dr. Myron Yaster as the first Guest Reviewer for PAAD. Myron needs no introduction. Most of you reading this newsletter will recognize him as one of the most well-respected and leading pediatric anesthesiologists in the history of our specialty. Today, he will review the origins of the 4-2-1 rule that has governed perioperative and hospital-based maintenance fluid therapy in children for decades.

The maintenance need for water in parenteral fluid therapy., HOLLIDAY MA, SEGAR WE. Pediatrics. 1957 May;19(5):823-32. PMID: 13431307
In this classic paper, Holliday and Segar proposed a simple-to-use formula that relates to the average caloric expenditure of a child of a given weight in kg:
- Infant up to 10 kg expend 100 kcal/kg;
- Children 10 – 20 kg expend 1000 kcal + 50 kcal/kg:
- Children > 20 kg expend 1500 kcal + 20 kcal/kg.The allowance of 50 mL/kg/24 hours will replace insensible losses and 66.7 ml/kg/24 hours will replace urinary losses so that 110 to 120 mL/100 kcal expended every 24 hours meets appropriate water maintenance needs. The math was further simplified as the “4-2-1 rule” and it is still used by anesthesiologists (and pediatricians) to this day. At the end of the article, Holliday and Segar conclude that daily electrolyte requirements for Na, Cl, and K are 3.0, 2.0, and 2.0 mEq/100 cal/day, respectively.
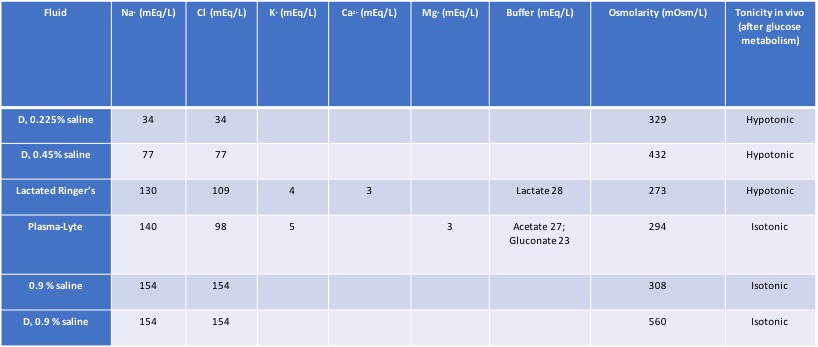
In a very important related and more recent paper, Ann Bailey and her colleagues point out “that these electrolyte requirements are theoretically met by the hypotonic maintenance fluid more commonly used in hospitalized children in the United States today, 5% dextrose with 0.2% normal saline. In Holliday and Segar’s original conclusions, it was emphasized that “these figures provide only maintenance needs for water. It is beyond the scope of this paper to consider repair of deficits or replacement of continuing abnormal losses of water.” Bailey adds, “Unfortunately, clinicians may often extrapolate the “4-2-1 rule” and the accompanying hypotonic solutions to clinical situations where they may not be appropriate and could, in fact, be harmful.”
Bailey et al. are spot on right! In the OR, we should ONLY be infusing isotonic solutions with Plasmalyte, Ringers Lactate, or (ab)normal saline. (I call it abnormal saline because there is nothing “normal” about it: it contains too much chloride and can produce a hyperchloremic metabolic acidosis). I believe we should always discontinue hypotonic solutions in the OR to avoid hyponatremia, a completely avoidable iatrogenic complication.
Because NPO times, particularly for liquids, continue to drop (it’s pretty clear it will or is already dropping to only an hour), and the risks of too much crystalloid are becoming increasingly clear, perhaps we need to rethink how much crystalloid we are infusing in the OR completely. We are almost certainly giving too much and in this era of ERAS, we probably should reconsider how we do this.
A last comment: Surprisingly, many of the trainees that I work with simply do not know the composition of most IV fluids. So, during the “boring” parts of an anesthetic I ask them to construct a table. This is what it should look like when done:
Posted on March 21, 2021, in Uncategorized. Bookmark the permalink. Leave a comment.

Leave a comment
Comments 0